
News
New Prescription: Ohio Valley Native Dr. Patrice Harris Is First Black Woman To Lead AMA
By: Aaron Payne | Ohio Valley ReSource
Posted on:
Dr. Patrice Harris took the oath in June to become the first African-American woman to serve as president of the powerful American Medical Association, the largest professional association for physicians in the United States.
Harris also brings another unique perspective to the job as someone who grew up in rural Appalachia.
“I was born and raised in Bluefield, West Virginia, in the heart of coal country,” Harris said. “My father worked on the railroad. My mother taught school. So I have a unique and personal connection and understanding of the region.”
She earned her undergraduate degree in psychology, a master’s degree in counseling psychology and medical degree from West Virginia University. Though she has long practiced psychiatry in Atlanta, Georgia, she keeps her connection to the region with regular home visits and by serving on the WVU Foundation board.

She has also served in leadership positions with the American Psychiatric Association, the Georgia Psychiatric Physicians Association, the Medical Association of Georgia, and The Big Cities Health Coalition.
Harris was elected last year to lead the AMA.
I recently spoke to her about what the appointment means to her, her ties to the Ohio Valley region, and how she thinks the AMA can help the region face some of the nation’s toughest health challenges.
Breaking Barriers
AARON PAYNE: What does it mean to you to be the first African-American woman elected as president of the AMA?
PATRICE HARRIS: It is certainly an honor and a privilege to be the first African-American woman president of the AMA. I know that I can stand as tangible evidence that young girls from communities of color can aspire not only to be physicians, but to be elected to the highest office of the physicians of this country.
PAYNE: What do you think it means to the AMA to have a woman of color as president?
HARRIS: Being president of the AMA is the culmination of many years of work, dedication and sacrifice. Not just from me, but by those who have been my supporters in the AMA, also my physician colleagues in psychiatry and from Georgia.
The president is the highest elected office of the AMA and is the primary spokesperson for the policies and the work of the AMA. I believe that the AMA is very proud, again of the work of all of its presidents, those proceeding me, but certainly there is some additional pride I believe in my currently being the first African-American woman to hold this office.
And not only that, for the first time the AMA will have women as the immediate past president, the president, and the president-elect, so that is another wonderful accomplishment that the AMA is celebrating.

HARRIS: The AMA is an organization that sets policy and then advocates for that policy on the federal level and certainly with the partners at the state level, for instance, the West Virginia State Medical Association.
We definitely highlight the burden, both the human cost and the financial cost of chronic disease. I know that in West Virginia, there is a significant burden for those who have diabetes, who have high blood pressure, those who have an opioid use disorder, so the AMA has strong policy.
We’ve been advocating for increased funding. We want to make sure we increase understanding that substance use disorder is a brain disorder. It’s a chronic illness just like diabetes and hypertension.
At the AMA, we’re strong supporters of the Affordable Care Act because we wanted to make sure that those who were uninsured or under-insured had access to healthcare. We know that in West Virginia, Kentucky and Ohio there are a significant number of folks who don’t have access to healthcare.
Certainly the expansion of Medicaid was critical in getting access to healthcare, so that people can go to their physicians and get treatment for their diabetes, and their hypertension, and their opioid use disorder. And get treatment early, so that they don’t feel like they have to wait until the disease has progressed, or that they don’t feel like the only option for care is the emergency department.
Strategic Arcs
Harris’ tenure finds her working to improve the health of patients and improve working conditions for doctors in an interesting time.
The Affordable Care Act, which the AMA supports, is again being debated in a federal appeals court over questions of its legality. The case is likely heading to the U.S. Supreme Court.
Her time will also be spent implementing and advocating for policies that fall under the AMA’s core strategic arcs: attacking dysfunction in the healthcare system, re-imagining medical education, and confronting the chronic disease crisis.
HARRIS: Regarding attacking the dysfunction in healthcare, we know that regulatory burdens, electronic health records are a significant cause of physician dissatisfaction and, unfortunately, burnout in the physician community. The AMA is working on several fronts to address that issue certainly to reduce the amount of paperwork and the regulatory burden. In fact, we did a study several years ago that showed that for every one hour physicians spend in caring for patients we spend two hours in [paperwork and desk work], and so we’re working on many fronts in that area.
We have been working on those areas for some time regarding changing and innovating the way we train the next generation of physicians. We have, over the last several years, awarded grants to medical schools first and now to graduate medical education programs. Those are the residency training programs that we physicians do after we graduate medical school. The AMA has awarded over $30 million dollars in grants to schools and other affiliated institutions to innovate and look at how we can all innovate in training the next generation of physicians.
https://www.youtube.com/watch?v=jkIGJ8_7gkQ
When it comes to decreasing the burden of chronic disease, we are working in the areas of pre-diabetes because we are imagining what we can do if we prevent people from getting type 2 diabetes. We are working in the hypertension space. We know that so many of us are walking around with high blood pressure and don’t know it. We’re working with physician practices to develop ways to make sure that folks who have high blood pressure are getting the treatment that they need, and certainly we know that then prevents later strokes and other health issues.
Of course as a psychiatrist, I’m highlighting the connection and the importance of incorporating mental health into overall health care, the importance of addressing trauma early on, so that we can prevent a disease burden related to trauma.
And finally, increasing the diversity of the physician workforce and amplifying the AMA’s new work on health equity.
Addiction Policy
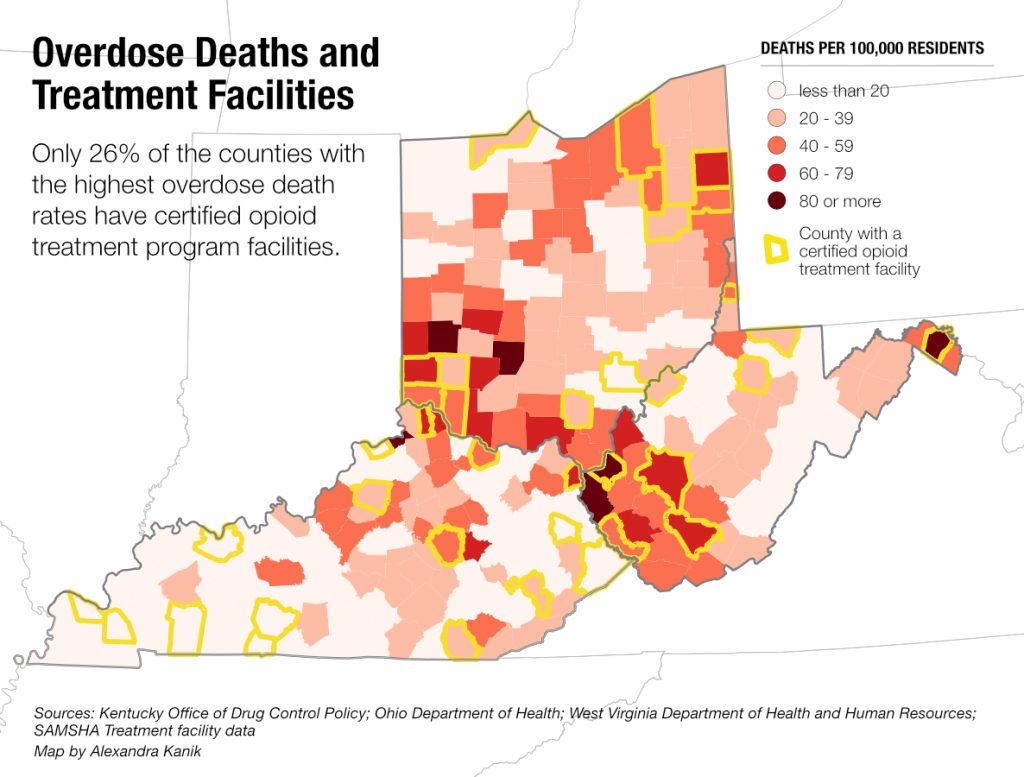
The Ohio Valley region has some of the highest fatal drug overdose rates in the nation. It was also considered a “canary in the coal mine” for the epidemic.
Opioid painkillers overprescribed by doctors and shipped in waves to “pill mills” by manufacturers and distributors fueled the addiction crisis in small, rural towns across the area.
The AMA’s Opioid Task Force that Harris chairs recently released its 2019 Progress Report on the epidemic. It highlights how improving doctor education about opioid painkillers and overprescription contributed to successful reductions. It also offers recommendations the AMA believes can break down barriers to treatment.
HARRIS: I think it is important to talk about what’s working. We highlight the numbers regarding the decreasing number of opioid prescriptions that are written, around 28 percent nationwide over the last four to five years. Physicians have been enhancing our education on opioid prescribing on pain, and so there is progress.
I do want to say, now we do want to be judicious in our prescribing, but we also don’t want to limit patients who have pain. We don’t want to limit their access to appropriate pain care and opioids do play a role in pain care.
There is an area [that can be improved upon] regarding access to treatment. Across this country, only 2 in 10 people who want opioid use disorder treatment have access to it.
We highlight the fact that there are more physicians and other health professionals who are trained to provide MAT, or medication assisted treatment. That’s the evidence-based treatment for those who have an opioid use disorder.
We need to make sure that we vigorously [minimize] regulatory burdens – we call those prior authorizations in our world. I may have to fill out a piece of paper or may have to make several phone calls before a patient can get into treatment. Well that delay in care could mean death, and so the AMA is highlighting that issue.
We work with several states also to make sure that state insurance commissioners are holding their insurers accountable for parity, making sure that coverage for substance use disorders and other mental disorders is on par, is the same, is at the same level as coverage for other medical illnesses.
Our progress report, as you note, highlights the progress that has been made and really points to areas where we need to continue to work. We can work with state regulators, and insurance commissioners, and attorneys general to make sure that barriers are eliminated.
PAYNE: Another recommendation made in the report is to lessen the burden of “step therapy,” where people with a substance use disorder will be required by insurance to try a certain treatment before they can be approved for another. In rural regions like ours where a treatment option may not be available, people are left with traveling miles and miles to get treatment. As advocates, how do you convince people making those decisions to take into account regions like ours?
HARRIS: The AMA always brings it back to the patient. We have to make sure that the patient is first and that the treatment options are based on what the patient needs, not what an insurance company has decided should be first. We always highlight the need to put the patient first, and take into account where the patient is, and the services available.
Regarding location, we need to make sure that services are available. We could use some innovation there. But you’re right, we should be looking at the patient, and the patient population, and the resources in making sure patients get what they need and not what’s on a piece of paper, or in an algorithm or in a step therapy document.
PAYNE: What do you see as the role of physicians in continuing to combat the opioid epidemic moving forward?
HARRIS: There are many complicated factors that lead us to where we are today in this opioid epidemic, but what we wanted to do [by forming the Opioid Task Force] was demonstrate physician leadership. You may be aware, our first set of recommendations came out in 2015, and those recommendations were specifically geared towards what physicians could do and it was to sign up for our state database programs.
You may be aware, or your listeners may be aware of the physician drug monitoring programs. Those are the programs where physicians can check to see what other medications, particularly opioids and other medications that might interact negatively with opioids. What other medications our patients are on? We encouraged our physicians to do that.
We encouraged in those first recommendations for physicians to enhance our education…and they did as evidenced by the progress report. Our second set of recommendations, as we discussed earlier, was about what can we all do as a community because physicians alone cannot solve this problem. It requires partnerships with state and federal government.
Mental Health
Harris plans to use her background as a psychiatrist to advocate for bringing mental health care into the primary health care system.
For rural areas like the Ohio Valley region where mental healthcare facilities can be scarce this will include making more mental health resources accessible.
Harris believes there are things that can be done to help this process along.
HARRIS: I am a child and adolescent psychiatrist, so certainly I’ve seen over the course of my career the importance of integrating mental health care into overall health care. For so many years there has been a stigma associated…with having a mental disorder, whether that’s depression, or bipolar, or schizophrenia, or a substance use disorder. Talking about it, elevating it in the conversation, bringing it into our primary care practices, there are many models to do that.
States and practices are using telemedicine, which means seeing patients through the use of computer and working with patients remotely. There are many models working. I believe New Mexico has a Hub and Spoke model, and again, not not just for mental health. There is innovation out there.
Actually, I keep in contact with the West Virginia University. I serve on the WVU Foundation and I’m back often. I know that in West Virginia they’ve been using, the psychiatry department, has been using telepsychiatry for many years.
Now it’s a matter of funding and making sure that those services are paid for in both our public and private payers. Again, a role that AMA plays in advocacy and of course a state medical association.
PAYNE: Is there anything you’d like to talk about that I didn’t ask about or anything additionally you’d like to add?
HARRIS: The only issue we haven’t talked about that I raised in my inaugural address was the need to focus on trauma and childhood trauma, ACES work. It stands for Adverse Child Experience Survey. We know that adults who experienced certain traumatic events in childhood are affected later…by cardiovascular disease, diabetes, heart disease.
The other issue that I just want to highlight, and I think we should talk more about in our country, is childhood trauma and the need to make sure that we have the resources available to address early socio-emotional learning in our children. And when our children have experienced trauma, we need to make sure there are systems in place to support them after they have experienced a trauma.